
ITB (Iliotibial band) injuries are a real worry for runners, and it’s not difficult to understand why. According to experts, the choices for dealing with this problem can be as extreme as surgery or even quitting running altogether.
When it comes to an ITB injury, they catch you by surprise. After just a few steps, the pain on the outer part of your knee can get intense, especially if you’re running downhill or going down steps. The best thing to do in this situation is to limit knee movement because the pain usually gets worse when you move. This is when you might see runners sidestepping downhill, allowing them to keep the painful knee as straight as possible.
Once the tendon becomes swollen and inflamed, the typical medical advice involves resting, applying ice, and using a compression bandage to handle the swelling. During the healing phase, it’s crucial to avoid activities like running or cycling since they can make the inflammation worse and set back your recovery.
Usually, it takes about 3 to 6 weeks for the knee to start feeling better. However, the challenge with ITB injuries is that it often comes back when you start to push yourself in your training routine. If it’s not on the same side, the pain might show up on the opposite leg. At this point, runners often turn to cortico-steroid injections, knee braces, and sometimes surgery – even though none of these really address the root cause of the injury!
Let’s take a closer look at what happens during an ITB injury.
The ITB (Iliotibial band) is essentially a robust strip of connective tissue that originates from the hip area and extends down the side of the thigh. It consists of three components: the fascia lata and its connections with the Gluteus Maximus and Tensor Fasciae Lata muscles. As it reaches the lower part, the ITB covers the bony prominence on the outer side of the thigh and extends to the lateral aspect of the kneecap.
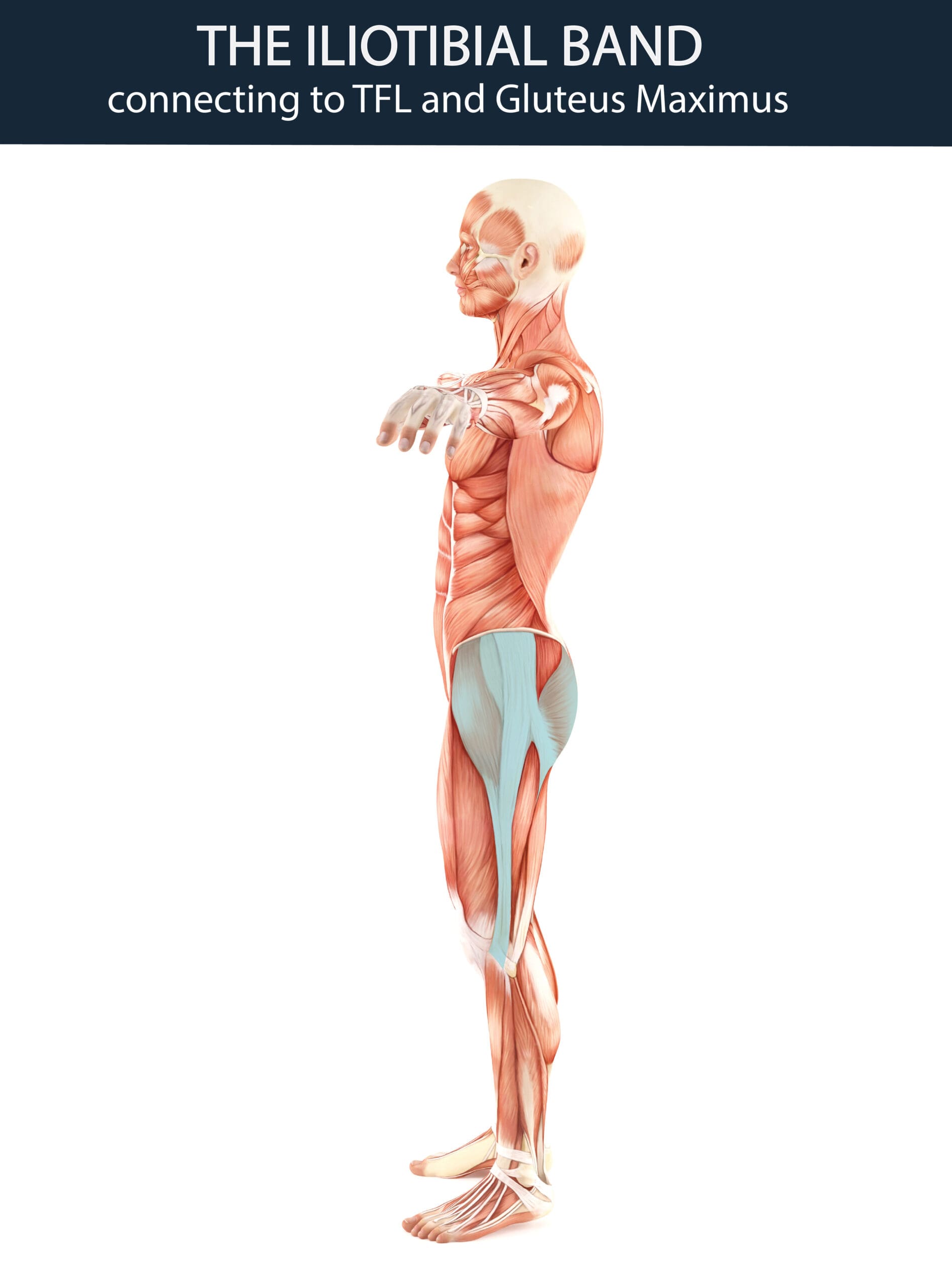
Its primary function is to work in conjunction with the TFL (Tensor Fasciae Lata), Gluteus Maximus, Medius and Minimus muscles to provide stability to the hip and knee during weight-bearing activities. However, maintaining a proper balance and coordination between the TFL and the Gluteus Maximus is crucial. Any disruption to this balance can lead to tightening and shortening of the ITB, causing it to rub against the bony prominence on the thigh. This friction can result in inflammation and discomfort and within a relatively short period compel the individual to limit physical activity.
How does the ITB become tight?
The TFL muscle takes on several roles in hip movement – it flexes, abducts, and internally rotates the hip. On the other hand, the Gluteus Maximus extends and externally rotates the hip. As a result, the TFL contributes to stability at the front of the hip, while the Gluteus Maximus ensures stability at the back. When both muscles work in tandem with the ITB, they also provide lateral stability to the knee.
However, if for some reason either of these two muscles becomes overly active, the surrounding fascia tightens, exerting a pull on the ITB, which leads to its tightening and shortening.
During running, as the hip undergoes internal and external rotation, these two muscles coordinate their actions in a rhythmic manner, ensuring a balance between movement and stability. Nonetheless, if disrupted movement patterns due to poor sitting or standing habits or previous injuries come into play, one of these muscles may become excessively engaged. This results in the tightening of the fascia around the muscle, leading to the shortening of the ITB. This issue extends beyond just causing irritation around the lateral epicondyle of the femur on the outside of the knee. A shortened ITB also triggers external rotation of the tibia and a lateral tilt of the patella, culminating in an abnormal alignment of the knee and added stress on the joint connecting the kneecap and the femur. Thus, while the symptoms may manifest around the knee area, the underlying problem originates from a flawed movement pattern that disrupts the equilibrium of hip rotation.
While rest, ice, and compression can alleviate the symptoms, they fail to address the core problem. This is why symptoms often resurface when an athlete resumes more intense running activities.
How does Lyno address this issue?
The answer lies in thoroughly assessing the whole body to pinpoint the movement pattern that’s causing the alignment issue. This pattern can come from any activity involving the TFL or Gluteus Maximus muscles. Both muscles are part of the body’s spiral movement patterns. Any habit that involves repeating spiral movements in one direction might overload and restrict the fascia around the involved muscles.
It could be an office worker who twists while sitting for long stretches, a mom carrying her baby on the same hip every day, someone pushing a stroller while favoring one side, or a runner who always takes a slanted route. These repetitive movements can strain the TFL or Gluteus Maximus, making the fascia tighten up defensively and affecting how the ITB works.

An example of a dysfunctional movement pattern that shortens the ITB –as recorded on the LYNO application
Once the therapist pinpoints the locked fascia pattern, the treatment is straightforward. They release the fascia, help you change the habit causing the issue, and gradually strengthen your body in a neutral position.
Dealing with an injury for the short term is relatively simple, but fixing recurring injuries means uncovering and tackling the root pattern. Once we figure out the puzzle of chronic injuries, the solution starts to become much clearer.